Axumin imaging-based guidance impacted clinical management and event-free survival
Journal of Urology (LOCATE study)
LOCATE study design
A prospective, US, multicenter, open-label study investigating the impact of Axumin® (fluciclovine F 18) PET/CT imaging on patient management of biologically recurrent prostate cancer after initial prostate cancer treatment and after negative or equivocal findings on standard-of-care imaging.1

Primary endpoint: The percentage of men with biochemical recurrence of prostate cancer following initial prior therapy whose clinical management was changed following an Axumin PET/CT scan as recorded by completed form stating their intended management before and after the scan, with any changes recorded.1
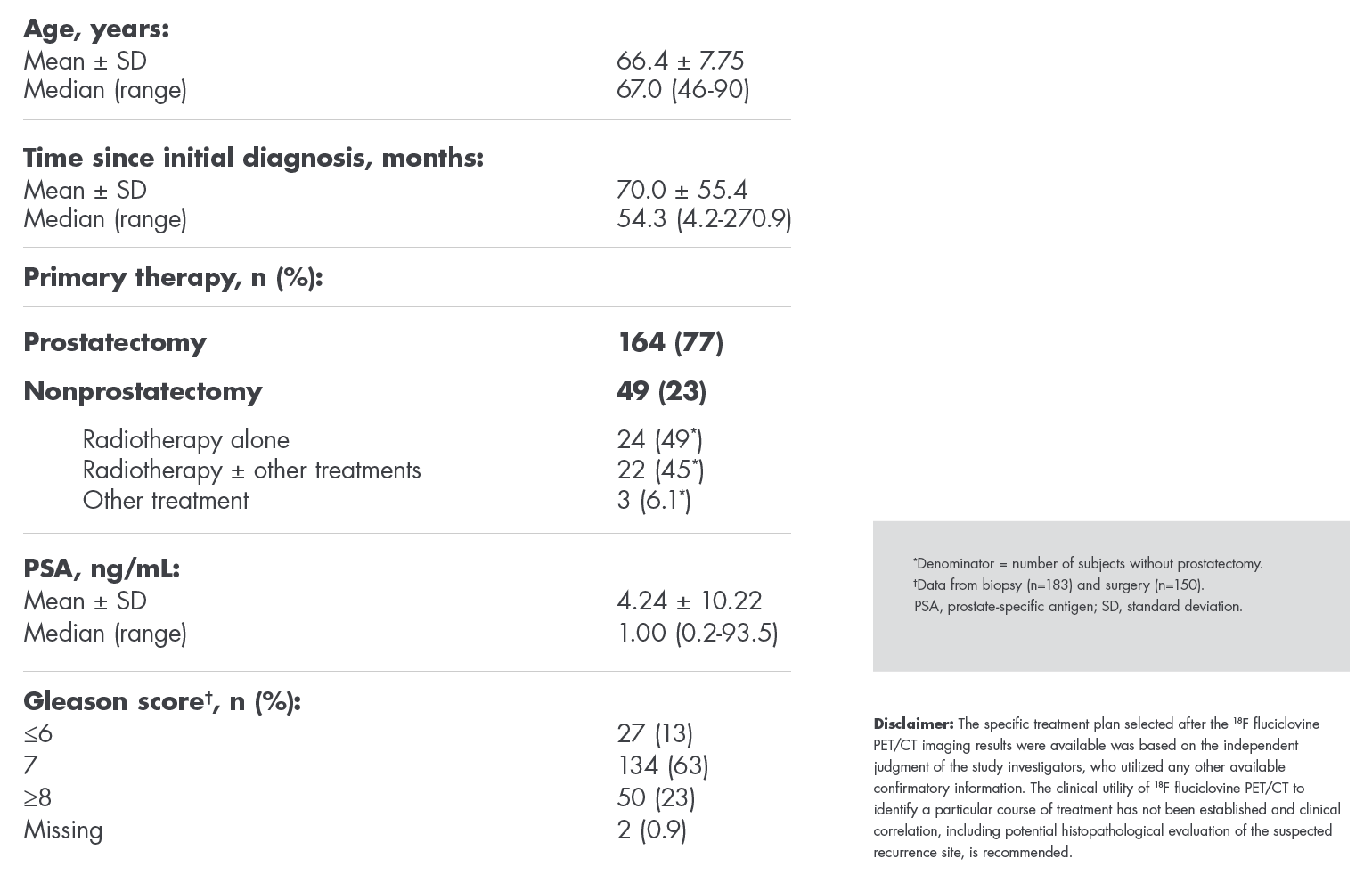
Patient Demographics1
Changes in approach for majority of patients
Overall change in management1
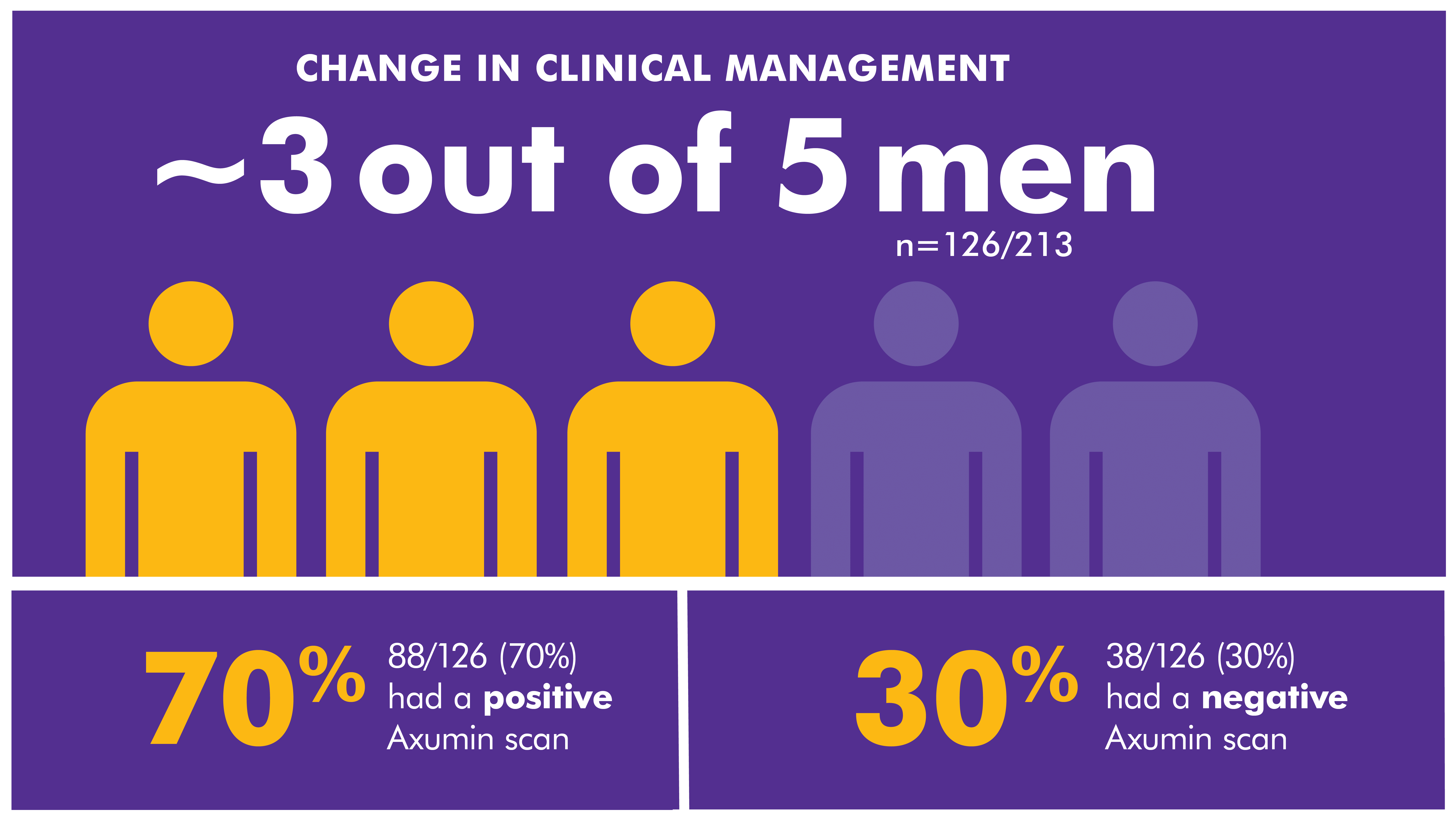
When presented with a negative or an equivocal scan, Axumin imaging may provide clarity for your decision-making1
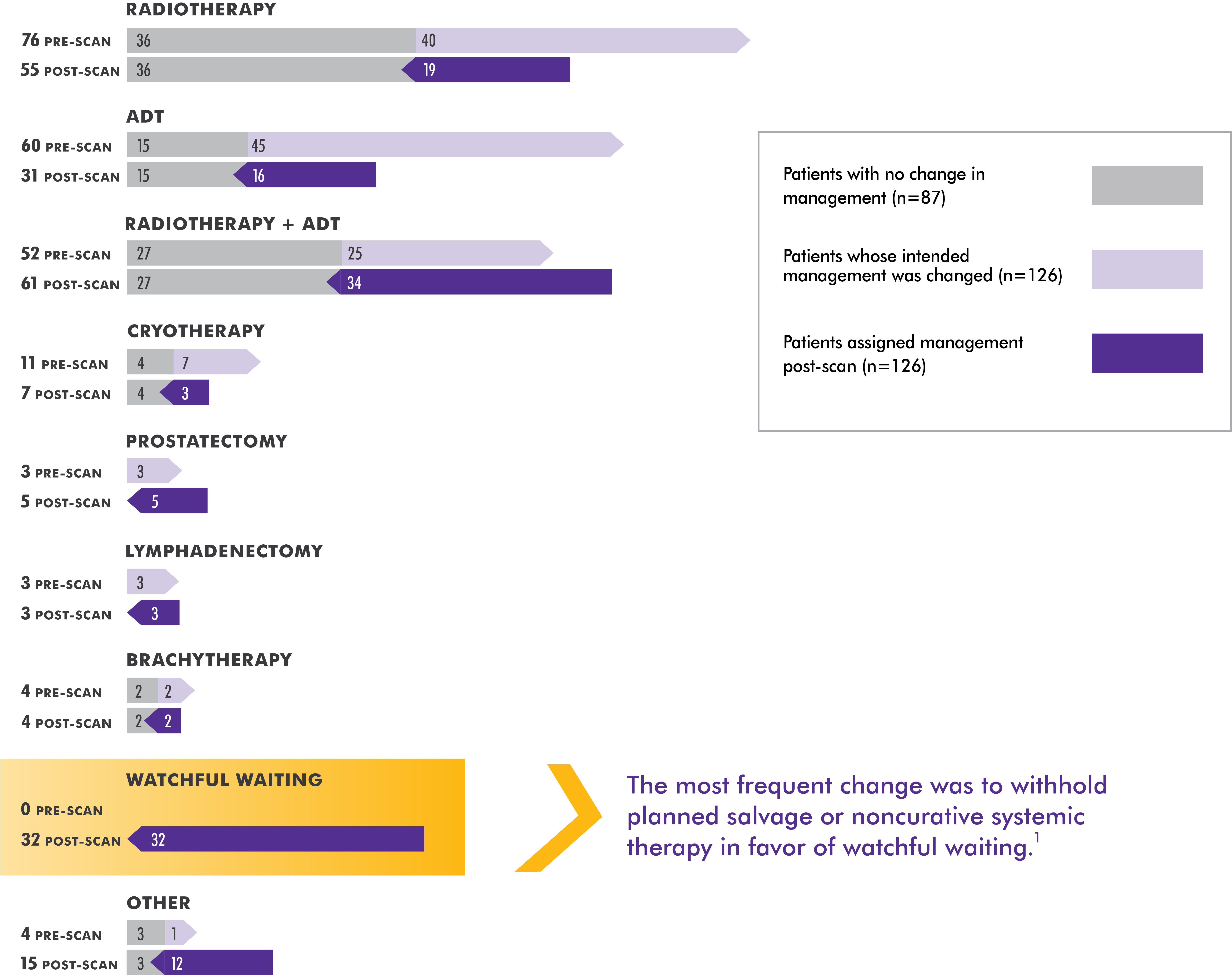
Changes seen across all management options
Change in approach based on results of Axumin scan1


Change in approach based on results of Axumin scan1
The specific treatment plan selected after the Axumin PET/CT imaging results were available was based on the independent judgment of the study investigators, who utilized any other available confirmatory information. The clinical utility of Axumin PET/CT to identify a particular course of treatment has not been established and clinical correlation, including potential histopathological evaluation of the suspected recurrence site, is recommended.
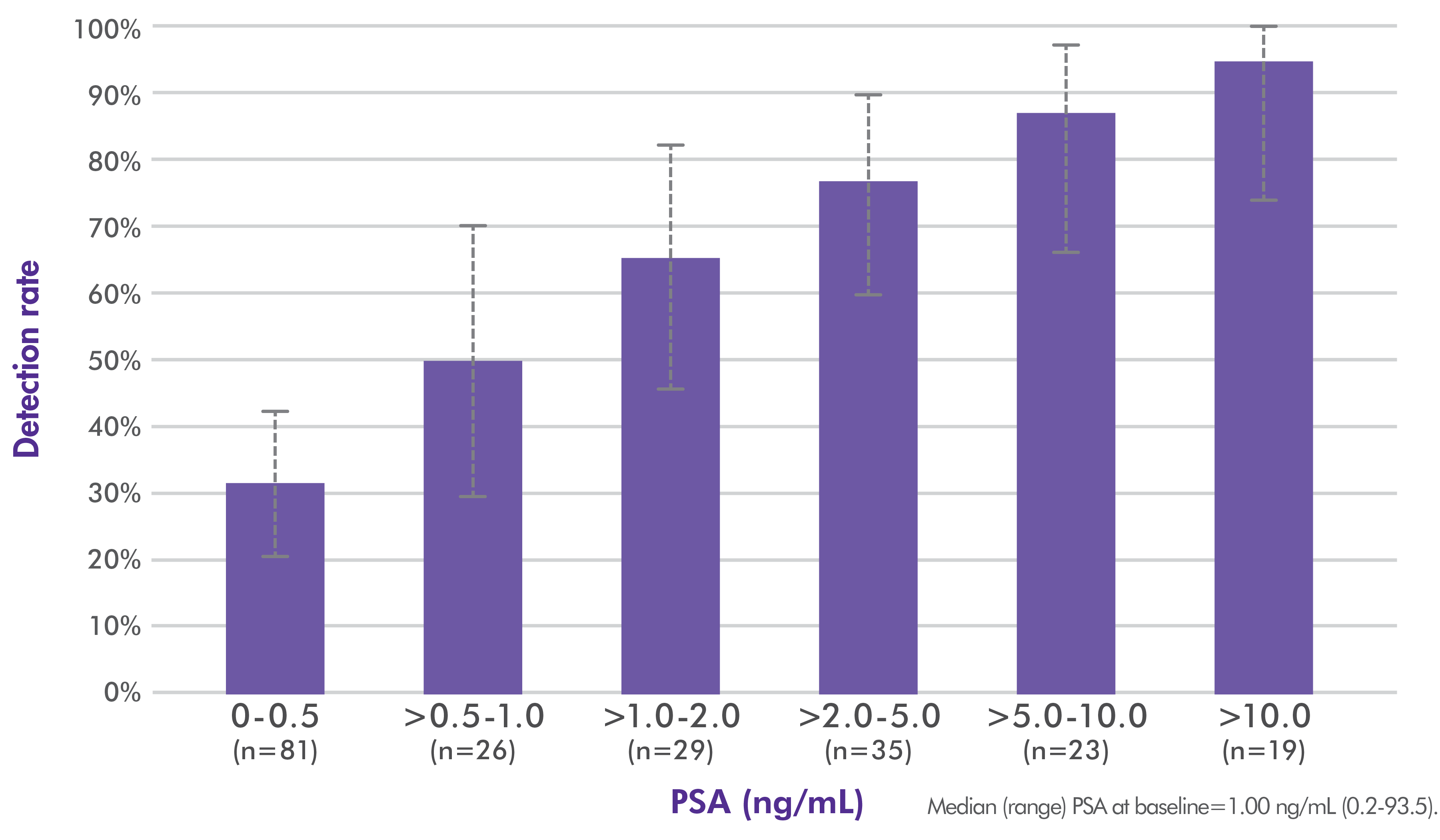
Positive findings on Axumin imaging even when PSA levels were ≤1.0 ng/mL
Detection rate increased as PSA level rose
Axumin-avid lesions were detected in 57% of patients (122/213) who had a negative equivocal finding on standard-of-care imaging, with 30% seen in the prostate or prostate bed and 38% outside (including 29% in lymph nodes, 2.3% soft tissues, and 11% bone).1
Axumin whole-body imaging detection rate by PSA level1
LOCATE Safety Data Consistent With Axumin Prescribing Information2
The safety profile of Axumin in the LOCATE trial was consistent with that described in the approved US Prescribing Information.
Lancet (EMPIRE-1 study)
The first prospective, randomized, controlled study to demonstrate that Axumin PET/CT-guided radiation therapy improved event-free survival rates3
A single-center, open-label, phase 2/3, randomized study comparing 3-year event-free survival in patients receiving radiotherapy based on conventional imaging vs Axumin PET/CT imaging. Eligible patients had adenocarcinoma of the prostate following prostatectomy, detectable PSA, and no systemic metastases on conventional imaging.3*
All patients underwent conventional imaging3

*Conventional imaging included a bone scan and either a CT or an MRI of the abdomen and pelvis.
Study endpoints and clinical measures3
Primary endpoint: 3-year event-free survival.
Event was defined as:
- PSA 0.2 ng/mL above post-XRT nadir followed by another higher value OR
- Persistent PSA, imaging or digital rectal examination failure OR
- Initiation of systemic therapy (including ADT) after XRT
Secondary endpoints: Impact of Axumin in post-prostatectomy radiotherapy decision-making, volumetric and dosimetric changes, and gastrointestinal and genitourinary toxicity.
Prespecified in treatment decision based on PET findings:
- Extrapelvic or skeletal uptake: radiotherapy aborted
- Pelvic nodal plus prostate uptake: radiotherapy administered to prostate bed and pelvis with boost† at site of uptake
- Prostate bed–only uptake: radiotherapy given to prostate bed
- No radiotracer uptake: prostate bed received radiotherapy
†The boost consisted of 45 to 50.4 Gy to pelvic nodes and 64.8 to 70.2 Gy to the prostate bed.
ADT, androgen deprivation therapy; CT, computed tomography; MRI, magnetic resonance imaging; XRT, radiation therapy.
Axumin scans demonstrated a high detection rate and impacted treatment decisions3
High detection rates across regions compared to conventional imaging3,4
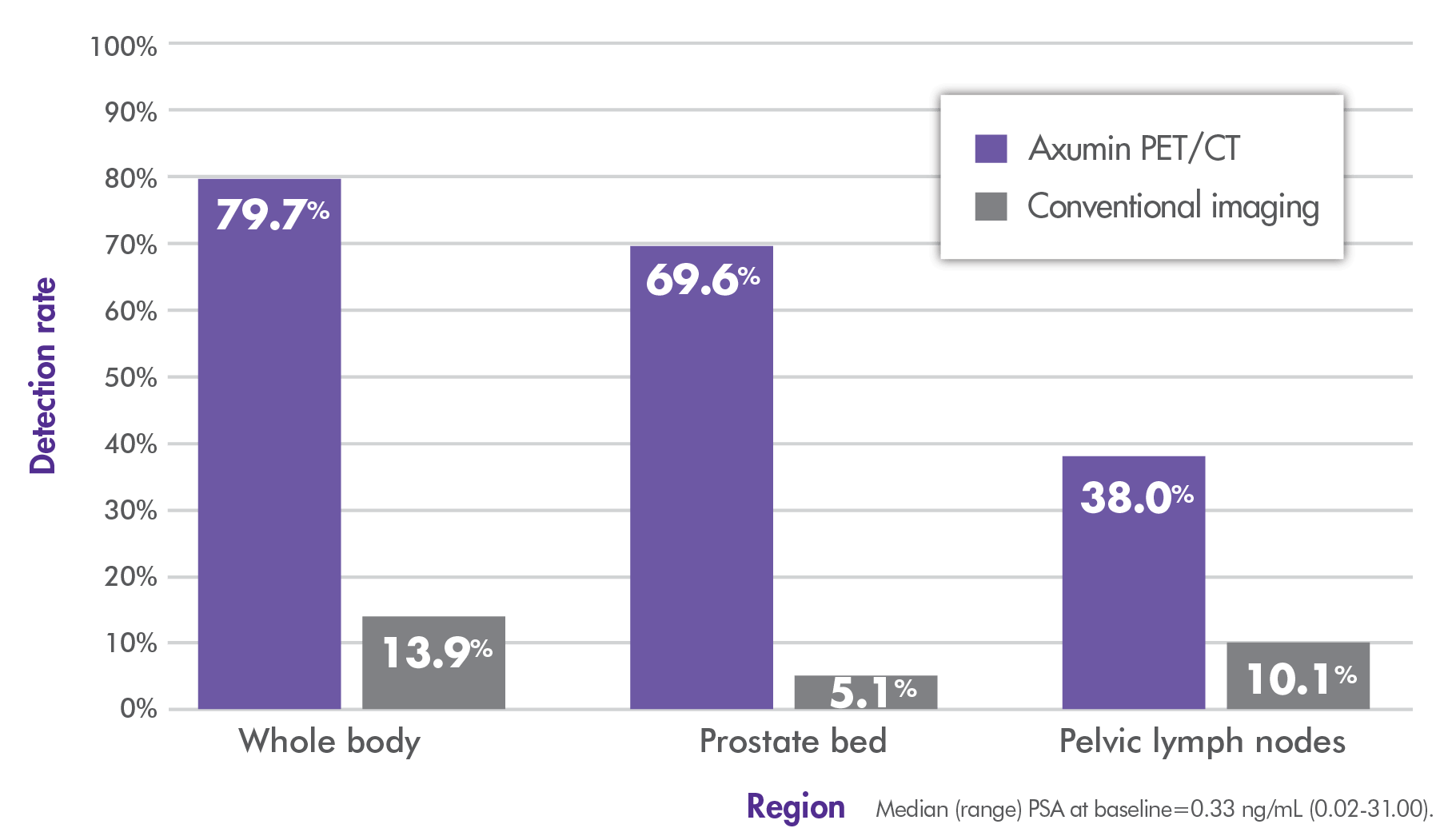
~80% overall (whole-body) detection rate with Axumin imaging vs 14% with conventional imaging.3,4
Axumin PET/CT changed clinical decision-making in more than one-third of patients
- 35.4% (28/79; P<0.001) of treatment decisions changed following imaging with Axumin3,4
- In the Axumin arm, 29.4% of patients with a PSA <0.5 ng/mL had radiotherapy decision changes4
- The radiotherapy field changed in 32% (24/75; P<0.001) of treatment plans3,4
- 14 patients had an expansion of the radiation field to include the prostate bed and pelvis
- 10 patients had a reduction in the radiation field to include the prostate bed only
Axumin-guided radiotherapy improved 3-year event-free survival3
- At year 3, patients whose treatment was guided by Axumin had a 12% improvement in event-free survival compared with conventional imaging: 75.5% vs 63%, respectively (P=0.0028)
- At year 4, the improvement in event-free survival was 24% (75.5% vs 51.2%; P<0.0001)
Event-free survival3

- Overall median follow-up was 3.52 years3
There were no significant differences in toxicity across both study arms3
References:
- Andriole GL, Kostakoglu L, Chau A, et al. The impact of positron emission tomography with 18F-Fluciclovine on the management of patients with biochemical recurrence of prostate cancer: results from the LOCATE trial. J Urol. 2019;201(2):322-331.
- Data on file. Blue Earth Diagnostics, Ltd. Oxford, UK.
- Jani AB, Schreibmann E, Goyal S, et al. 18F-fluciclovine-PET/CT imaging versus conventional imaging alone to guide postprostatectomy salvage radiotherapy for prostate cancer (EMPIRE-1): a single centre, open-label, phase 2/3 randomised controlled trial. Lancet. 2021:S0140-6736(21)00581-X.
- Abiodun-Ojo OA, Jani AB, Akintayo AA, et al. Salvage radiotherapy management decision in post-prostatectomy patients with recurrent prostate cancer based on 18F-fluciclovine PET/CT guidance. J Nucl Med. 2021:jnumed.120.256784. doi: 10.2967/jnumed.120.256784. Epub ahead of print.
Abbreviation: ADT, androgen deprivation therapy.
INDICATION
Axumin® (fluciclovine F 18) injection is indicated for positron emission tomography (PET) imaging in men with suspected prostate cancer recurrence based on elevated blood prostate specific antigen (PSA) levels following prior treatment.
IMPORTANT SAFETY INFORMATION
- Image interpretation errors can occur with Axumin PET imaging. A negative image does not rule out recurrent prostate cancer and a positive image does not confirm its presence. The performance of Axumin seems to be affected by PSA levels. Axumin uptake may occur with other cancers and benign prostatic hypertrophy in primary prostate cancer. Clinical correlation, which may include histopathological evaluation, is recommended.
- Hypersensitivity reactions, including anaphylaxis, may occur in patients who receive Axumin. Emergency resuscitation equipment and personnel should be immediately available.
- Axumin use contributes to a patient’s overall long-term cumulative radiation exposure, which is associated with an increased risk of cancer. Safe handling practices should be used to minimize radiation exposure to the patient and health care providers.
- Adverse reactions were reported in ≤1% of subjects during clinical studies with Axumin. The most common adverse reactions were injection site pain, injection site erythema and dysgeusia.
To report suspected adverse reactions to Axumin, call 1-855-AXUMIN1 (1-855-298-6461) or contact FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
Please see Axumin full Prescribing Information.